Patient History: A 68-year-old patient with systemic lupus erythematosus (SLE) has been referred for the evaluation of an asymptomatic right atrial mass found on an outside cardiac echocardiogram.
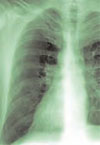
Salient findings: SSFGRE cardiac gated magnetic resonance and computed tomography of the heart with contrast demonstrate a large (3 cm x 4.5 cm) fusiform aneurysm of the right coronary artery (RCA). This should account for the atrial mass seen on the outside echocardiogram. Although there is marked circumferential mural thrombus (see horizontal arrows in Figs. 1 and 2, above), the vessel lumen is widely patent (see vertical arrows in Figs. 1 and 2, above), as evidenced by free flow of contrast within the center of the RCA.
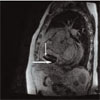
Figure 2: SSFGRE coronal MRI
Figure 2: SSFGRE coronal MRI

Figure 1: Coronary CT angiogram
Figure 1: Coronary CT angiogram
Patient population and natural history of disease: Coronary artery aneurysms are defined as dilatation of the artery to greater than 1.5% to 2.0% of the normal artery diameter; however, they can be much larger. Coronary artery aneurysms are rare, occurring in 1.4 to 2.0% of the general population and in up to 5.3% of those undergoing cardiac catheterization. In North America, the most common etiology of coronary artery aneurysms is atherosclerosis. In Japan, the most common cause is likely Kawasaki disease. Other etiologies include congenital connective tissue diseases such as Marfan syndrome and Ehlers-Danlos syndrome, dissection, infections such as syphilis, vasculitis, and post-coronary intervention. The RCA is most commonly involved, followed by the left anterior descending artery (LAD). Consequences include thrombus formation and rupture with subsequent infarction, ischemia, and/or tamponade. SLE may be the culprit in this patient’s RCA aneurysm.
Management: Coronary artery aneurysms are often diagnosed incidentally, and rupture is rare. If symptoms of ischemia or impending rupture occur, bypass can be performed in selected patients. Some physicians advocate surgery in all patients with aneurysms that are greater than three to four times the normal native vessel diameter. Studies are limited, however, and treatment is often based on anecdotal evidence. Without symptoms and with a widely patent vessel lumen, as in this patient, many would advocate medical management with an antiplatelet +/- anticoagulant regimen. Some studies have shown an association of abdominal aortic aneurysm (AAA) in patients with coronary artery aneurysms and, therefore, advocate screening for AAA in these patients.
Take-home points:
- Coronary artery aneurysms are typically found incidentally, and rupture is rare;
- Surgery is indicated for symptoms of cardiac ischemia or in cases where there is concern for impending rupture; and
- Coronary artery aneurysms are associated with atherosclerosis, Kawasaki disease, connective tissue diseases, and post-coronary interventions. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine in Rochester, Minn.
References
- Collins MJ, Borges AJ, Singh G, et al. A giant coronary artery aneurysm in the right coronary artery. Cardiovasc Pathol. 2006 May-Jun;15(3):150-152.
- Mariscalco G, Mantovani V, Ferrarese S, et al. Coronary artery aneurysm: management and association with abdominal aortic aneurysm. Cardiovasc Pathol. 2006 Mar-Apr;15(2):100-104.