A recent HealthGrades Quality Study titled Patient Safety in American Hospitals (July 2004) highlighted the frequency of patients dying from complications that develop while in hospitals. Failure to rescue, according to the 3-year study, accounts for 60,000 deaths each year in Medicare patients under the age of 75.
Based on my experience as a pulmonary and critical care physician, this statistic quantifies an important problem. Deaths from complications of illness, or care, during a hospital stay happen more than we’d like to admit. However, the good news is that by identifying the underlying problem and deploying some targeted, systemic changes, hospitalists can begin to handle decompensation quickly, proactively, and before it’s too late.
Moving forward, hospitals need to build an effective patient safety net, which requires three important elements: point-of care tools for caregivers, proactive clinical surveillance, and real-time process monitoring.
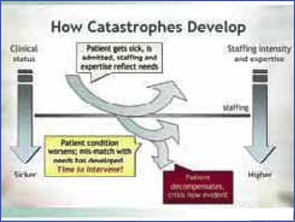
FIGURE 1. Catastrophe Timeline — Review of the patient’s chart revealed instability had been developing for hours before a “code” was called
Reasons for Failure to Rescue
A huge effort, and amount of money, has been focused on finding errors that lead to harm. Unfortunately, we’re tackling the wrong errors. New tools like barcode medication administration or CPOE tackle errors of commission. These errors might occur when a doctor or nurse administers a wrong dose or wrong medication. Errors of commission are much easier to identify and solve, but clinically significant errors of commission that cause harm are relatively rare events and don’t affect overall hospital mortality.
Errors of omission, however, are much more insidious. An error of omission is an error that occurs when an action is not taken or an important step in the process is left out. Examples of an error of omission include sub-optimal patient care resulting from the inadequate availability of patient information for decision-making, or a more blatant example, when a patient’s vital signs indicate decompensation but the clinical response is inadequate or delayed.
Errors of omission continue in today’s hospitals for two very important reasons: First, we lack a systematic way to handle clinical decompensation. While we have “code” teams, their efforts often come into play too late. Second, lacking a way to recognize and respond to the issue, we have accepted that failure to rescue is in some ways inevitable and excusable.
The basic, first step is to replace the inherently unreliable paper patient chart. Paper patient charts get misplaced, information is sometimes missing and/or illegible, and they make it impossible for a team effort to optimize care.
Hospitals need to get patient data such as vital signs and medication usage in electronic form. That way, it is effortless and time-efficient to determine a patient’s status and check up on patients even when not physically near them. Making this change alone, even in only one hospital unit, hospitalists can begin to effect significant positive changes in patient safety outcomes.
Catastrophes Aren’t Inevitable
Often, the first time physicians become aware of a problem is when they receive a frantic call to come to the bedside. The patient is decompensating and needs immediate, dramatic intervention to save their life. However, when we take the time to look back at the patient chart and “connect the dots,” we see that instability had been developing for hours before an urgent summons for assistance.
Even with the best care, patients’ clinical needs often change after admission. Patient status can change rapidly, so a perfect assessment earlier in the day can quickly become dated. Further, bedside staff have many other patients, and staffing assignments don’t build in “slack time” to permit paying extra attention when problems develop. Consequently, signs of clinical deterioration are often missed or not acted upon until there’s a code on the unit and dramatic measures are needed to save a life.