Under the Microscope: Medication Reconciliation

click for large version
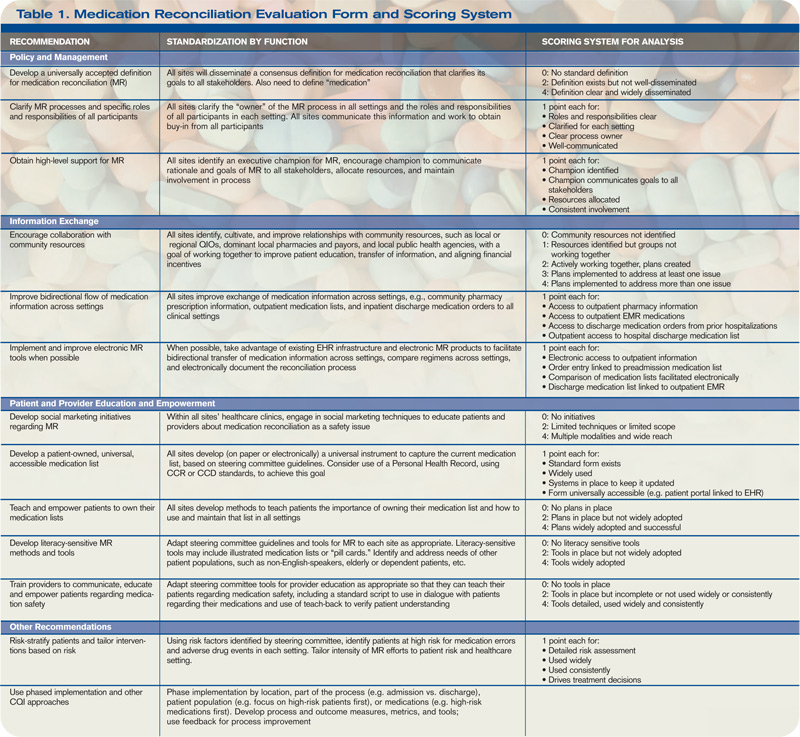
Table 1. Medication Reconciliation Evaluation Form and Scoring System
click for large version
Table 1. Medication Reconciliation Evaluation Form and Scoring System

There may be ways to serve up the discharged medication list in a patient-friendly way using some IT or an image library of medications. … I do not foresee a medication reconciliation IT application, unfortunately.—Jeffrey Schnipper, MD, MPH, FHM, Brigham and Women’s Hospital, Boston
Boston hospitalist Jeffrey Schnipper, MD, MPH, FHM, is no stranger to quality initiatives aimed at medication reconciliation (MR). His research at Brigham and Women’s Hospital and Massachusetts General Hospital revealed a potential reduction of serious medical errors per patient to 0.3 from 1.4 in the past four years.
“I think those are achievable results,” he says. “This is all about doing those things better than we were always doing before.”
Now Dr. Schnipper will work to bring similar results to hospitals across America as principal investigator for SHM’s three-year, multicenter, MR quality-improvement study. The study, funded by a $1.5 million grant from the Agency for Healthcare Research and Quality (AHRQ), will develop a database to research the best practices in MR and provide a mentored implementation model for other hospitals to use.
The project also will include a package of materials and tools adaptable for any hospital, as well as an implementation guide with the mentored implementation model. “It really should be everything a site needs to improve its MR process,” says Dr. Schnipper, director of clinical research at the Brigham and Women’s Hospital Hospitalist Service and assistant professor at Harvard Medical School.
According to The Institute for Safe Medication Practices, MR is the process of comparing a patient’s medication orders with their previously prescribed medication regimen and communicating any necessary changes to patients and their next providers of care. More than 1.3 million medication errors occur annually in the U.S.; MR has been shown to eliminate as many as half of those errors and 20% of adverse medical events.
JoAnne Resnic, MBA, BSN, RN, senior project manager at SHM, says SHM will use the grant to fund research investigators, SHM’s project staff, and the development of a database for each of the study’s six sites to house their data collection and provide site-specific progress reports throughout the course of the study. SHM is working with consultants and physician co-investigators, a steering committee of nationally recognized thought leaders in medication reconciliation, a research pharmacist, and others to “help us take a pretty deep dive into the process and, hopefully, explain why some interventions work in some places and why they may not in others,” Resnic says.
According to Dr. Schnipper, SHM will conduct an interrupted time series at the sites, collecting baseline data for six months at each, then for 21 months after interventions begin. The study specifically will address 13 facets of medication reconciliation, scoring the facets based on their effectiveness (see Table 1, p. 6).
Each facet will be re-evaluated when different parts of the intervention are turned on, which should reveal “the most active ingredients that correspond to improved outcomes,” he says.
Dr. Schnipper emphasizes that there are two integral facets for improving MR: patient education and access to preadmission medication sources. Technology could be an answer to advancing these components, but it is not the sole link. “There may be ways to serve up the discharged medication list in a patient-friendly way using some IT or an image library of medications to help patients,” he says. “I do not foresee a medication reconciliation IT application, unfortunately.”



