Medical malpractice and the hospitalist: Reasons for optimism
Fear of malpractice litigation weighs on many physicians, including hospitalists. Specific concerns that physicians have about facing a malpractice claim include stigmatization, loss of confidence in one’s own clinical skills, and a possible personal financial toll if an award exceeds the limit of one’s malpractice insurance.
Physician worries about malpractice are increasingly being raised during discussions of burnout, with a recent National Academy of Medicine discussion paper listing malpractice concerns as a possible factor that could contribute to physician burnout.1
Dr. Adam C. Schaffer
In addition to physician concerns about malpractice-related stigma, payment of a malpractice claim triggers reporting requirements. Among the organizations to which paid malpractice claims must be reported is the National Practitioner Data Bank, which is a government-run database of all malpractice payments made on behalf of individual physicians that can be queried by health care organizations as part of the credentialing process. Although the information in the National Practitioner Data Bank is not accessible to patients, a number of states – 17 in one published tally2 – maintain websites providing publicly available information on individual physicians’ malpractice history.
Malpractice fears also influence physician behavior generally, leading to defensive medicine, though the actual costs of defensive medicine are debated. A national survey of physicians by Bishop and colleagues found that 91% felt that physicians order more tests and procedures than patients require in order to try to avoid malpractice claims.3 A survey of 1,020 hospitalists asked what testing they would undertake when provided clinical vignettes involving preoperative evaluation and syncope.4 Overuse of testing was common among hospitalists, and most hospitalists who overused testing specified that a desire to reassure either themselves or the patient or patient’s family was the reason for ordering the unnecessary testing.
The extent to which this overuse was driven by liability fears specifically is not clear. Overuse of testing was less common among physicians associated with Veterans Affairs Hospitals, who generally are not subject to personal medical malpractice liability. But a history of a prior malpractice claim was not associated with significantly greater overuse in the survey.
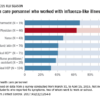
Hospitalists’ concerns about medical liability notwithstanding, data on the absolute malpractice risk of hospitalists and current trends in medical liability are both encouraging. An important source of our understanding about the national medical malpractice landscape is CRICO Strategies National Comparative Benchmarking System (CBS), which includes the malpractice experience from multiple insurers and represents 400 hospitals and 165,000 physicians. A December 2014 analysis of cases involving hospitalists from the CBS database showed that the malpractice claims rate for hospitalists was lower than those for other comparable groups of physicians.5 Hospitalists (in internal medicine) had a claims rate of 0.52 claims per 100 physician coverage years, which was significantly lower than the claims rate for nonhospitalist internal medicine physicians (with a rate of 1.91 claims per 100 physician-coverage years) and for emergency medicine physicians (with a rate of 3.50 claims per 100 physician-coverage years).

Dr. Allen Kachalia
The most common types of malpractice allegations made against hospitalists were related to medical treatment, diagnosis, and medications. Medication-related allegations made up almost 10% of claims against hospitalists, and a recent CRICO Benchmarking Report on medication-related malpractice claims found that the most common classes of medications involved in claims against hospitalists were anticoagulants, analgesics, and antibiotics.6 Payment was made in about one-third of hospitalist cases, which is similar to other specialties. Among hospitalist cases in which a payment was made, the mean payment was $384,617, which is comparable to other inpatient paid claims, though significantly higher than the average payment on outpatient claims.
A remarkable national trend in medical malpractice, based on an analysis of data supplied by the National Practitioner Data Bank, is that the overall rate of paid claims is decreasing. From 1992 to 2014, the overall rate of paid claims dropped 55.7%.7 To varying degrees, the drop in paid claims has occurred across all specialties, with internal medicine in particular dropping 46.1%. The reason for this decrease in paid claims is not clear. Improvements in patient safety are one possible explanation, with tort reforms also possibly contributing to this trend. An additional potential factor, which will likely become more important as it becomes more widespread, is the advent of communication and resolution programs (also known as disclosure, apology, and offer programs).
In communication and resolution programs, the response to a malpractice claim is to investigate the circumstances surrounding the adverse event underlying the claim to determine if it was the result of medical error. When the investigation finds no medical error, then the claim is defended. However, in cases in which there was a medical error leading to patient harm, then the error is disclosed to the patient and family, and an offer of compensation is made.
One of the most prominent communication and resolution programs exists at the University of Michigan, and published experience from this program shows that, after implementation of the program, significant drops were seen in the number of malpractice lawsuits, the time it took to resolve malpractice claims, the amount paid in patient compensation on malpractice claims, and the costs involved with litigating malpractice claims.8 One of the goals of communication and resolution programs is to utilize the information from the investigations of whether medical errors occurred to find areas where patient safety systems can be improved, thereby using the medical malpractice system to promote patient safety. Although the University of Michigan’s experience with its communication and resolution program is very encouraging, it remains to be seen how widely such programs will be adopted. Medical malpractice is primarily governed at the state level, and the liability laws of some states are more conducive than others to the implementation of these programs.
Hospitalist concerns about medical malpractice are likely to persist, as being named in a malpractice lawsuit is stressful, regardless of the outcome of the case. Contributing to the stress of facing a malpractice claim, cases typically take 3-5 years to be resolved. However, the risk for hospitalists of facing a medical malpractice claim is relatively low. Moreover, given national trends, hospitalists’ liability risk would be expected to remain low or decrease moving forward.