Trump, not health care, likely focus of midterm elections
Come November 2018, Americans will return to the polls to vote for their representatives in Congress, for governors, and for state legislative seats.
Dr. Robert Berenson
Health care has been a topic of debate since the 2016 elections brought a Republican sweep to the executive and legislative branches, but other issues have since moved to the forefront. Will the midterm elections this year prove health care to be a significant issue at the polls?
Unlikely, said Robert Berenson, MD, FACP, Institute Fellow of the Health Policy Center at the Urban Institute. More likely, the election will be a referendum on President Donald Trump, he said. “Things are so partisan right now and it’s all about Trump. I don’t see serious discussion about health policy.”
Ron Greeno, MD, MHM, FCCP, immediate past president of SHM and former chair of the Public Policy Committee, also doesn’t see health care rising to the top of election year issues. But that doesn’t mean health care doesn’t matter to American voters.
“Whether Democrats control the House or Republicans control the House won’t likely make a big difference in terms of impact on the things we care about,” said Dr. Greeno. “The issues they debate in Washington are not going to save the health care system. They are just debating about who is going to pay for what and for whom. To save our health care system, we have to lower the cost of care and only providers can do that.”

Dr. Ron Greeno
What the government can do, he said, is create the right incentives for providers to move away from fee for service and participate in new models that may lower the cost of care. At the same time, “the economy also has to grow at a robust pace, which will make a huge difference. So, recent increases in economic growth rate are welcomed,” said Dr. Greeno.
In 2015, Republicans and Democrats came together to pass bipartisan legislation aimed at moving the health care system away from fee for service: the Medicare and CHIP Reauthorization Act, or MACRA.
However, the law has not been without frustrations, and these concerns will likely not be part of any candidate campaigns in 2018, Dr. Greeno predicted: “There’s not a lot of appetite to reopen the statute (more than) 2 years after it passed.”
MACRA provides clinicians two pathways to reimbursement. The first track, called MIPS (Merit-Based Incentive Payment System), bases a portion of physician reimbursement on scores measured across several categories, including cost and quality. It still operates largely under a fee-for-service framework but is meant to be budget neutral; for every winner there is a loser.
The second track, called the APMs (Alternative Payment Models), requires physicians to take on substantial risk (with potential for reward), if they can achieve specific patient volumes under approved models. However, few providers qualify, especially among hospitalists, though the structure of the program makes it clear that the Centers for Medicare & Medicaid Services intends to have most providers ultimately transition to APMs.
“There’s growing recognition that MACRA, at least the MIPS portion, was a big mistake but Congress can’t go back and say we blew it,” Dr. Berenson said. “CMS has now exempted somewhere between 550,000 and 900,000 clinicians from MACRA,” because they cannot meet the requirements of either pathway without significant hardship.1
CMS wasn’t considering hospitalists specifically when implementing the law, though hospitalists admit half of the Medicare patients in the United States, Dr. Greeno said. There are very few hospitalists currently participating in Advanced APMs and those that are, do not see the volume of patients the pathway requires.
“What hospitalists do is very conducive to alternative payment models, and we can help those alternative payment models drive improved quality and lowered costs,” said Dr. Greeno. “Hospitals use hospitalists to help them manage risk, so it’s frustrating that most hospitalists will not meet the thresholds for the APM track and benefit from the incentives created.”
However, the Society of Hospital Medicine continues to work on behalf of hospitalists. Thanks to its efforts, Dr. Greeno explained, CMS is planning in 2019 to allow hospitalists to choose to be scored under MIPS based on their hospital’s performance across reporting categories. Or, they can choose to report on their own and opt out of this new “facility-based” option.
“We are working with (CMS) to figure out how to make this new option work,” said Dr. Greeno.
At the state level, 36 governorships are up for grabs and those outcomes could influence the direction of Medicaid. In Kentucky, the Trump administration approved a waiver allowing the state to enforce work requirements for Medicaid recipients. However, on June 29, 2018, the D.C. federal district court invalidated the Kentucky HEALTH waiver approval (with the exception of Kentucky’s IMD SUD [institutions for mental disease for substance use disorders] payment waiver authority) and sent it back to HHS to reconsider. Ten other states as of August 2018 had applied for similar waivers.2 However, Dr. Berenson believes that most of what could happen to Medicaid will be a topic after the midterm elections and not before.
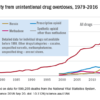
He also believes drug prices could become an issue in national elections, though there will not be an easy solution from either side. “Democrats will be reluctant to say they’re going to negotiate drug prices; they’re going to want the government to negotiate for Medicare-like pricing.” Republicans, on the other hand, will be reluctant to consider government regulation.
As a general principle leading into the midterms: “Democrats want to avoid an internal war about whether they are for Medicare for all or single payer or not,” Dr. Berenson said. “What I’m hoping doesn’t happen is that it becomes a litmus test for purity where you have to be for single payer. I think would be huge mistake because it’s not realistic that it would ever get there.”
However, he cites an idea from left-leaning Princeton University’s Paul Starr, a professor of sociology and public affairs, that Democrats could consider: so-called Midlife Medicare, an option that could be made available to Americans beginning at age 50 years.3 It would represent a new Medicare option, funded by general revenues and premiums, available to people age 50 years and older and those younger than 65 years who are without employer-sponsored health insurance.
Regardless, as the United States catapults toward another election that could disrupt the political system or maintain the relative status quo, Dr. Greeno said hospitalists continue to play key roles in improving American health care.
“There are programs in place where we can get the job done if we in the provider community are creative and participative,” he said. “Some of the most important work being done is coming out of the CMS Innovation Center. Hospitalists continue to be a big part of that, but we knew it would take decades of really hard work and I don’t see anything happening in the midterms to derail this or bring about a massive increase in the pace of change.”
References
1. Dickson V. CMS gives more small practices a pass on MACRA. Modern Healthcare. Published June 20, 2017.
2. Medicaid Waiver Tracker: Which States Have Approved and Pending Section 1115 Medicaid Waivers? Kaiser Family Foundation. Published Aug. 8, 2018.
3. Starr P. A new strategy for health care. The American Prospect. Published Jan. 4, 2018. Accessed March 5, 2018.