SHM has heard anecdotes from hospitalists that, post-COVID-19 pandemic, the culture around paid time off (PTO) has been shifting—both in prevalence and in use. Some groups are exploring PTO policies due to local regulations, while others are using it to promote well-being among their teams.
In response, SHM has examined PTO from several perspectives to gain a deeper understanding of the current state in hospital medicine and to anticipate where the field may be headed.
The 2024 Hospital Medicine Workforce Experience Report indicated that hospitalists with access to PTO were more likely to meet the criteria for professional fulfillment and less likely to meet the criteria for burnout. This highlighted the importance of time off as a tool to promote wellness in hospital medicine.
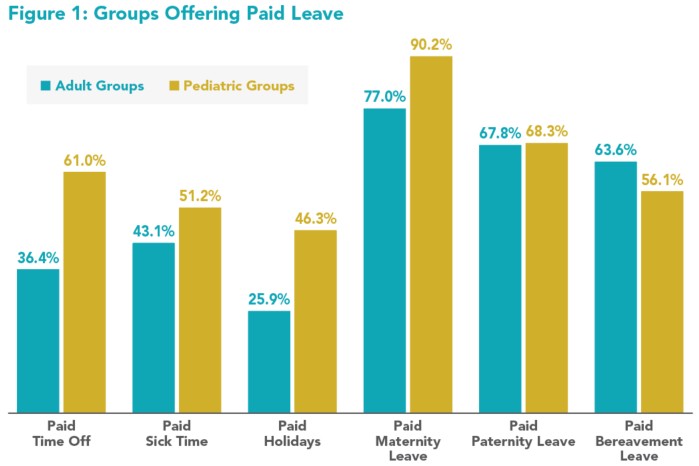
The 2025 State of Hospital Medicine (SoHM) Report, however, found that only about a third of adult hospitalists received PTO, which is only a slight increase from the 2023 SoHM. The 2025 SoHM Report additionally explored the various types of paid leave offered to adult and pediatric groups and found that adult groups are trailing pediatric groups in offering paid leave (see Figure 1 above).
On October 29, 2025, SHM’s Practice Management Webinar Series hosted a panel discussion entitled “Just Give Me a Break! Navigating Time Off for Hospitalists.” The webinar underscores that PTO and time-off policies are driven by the unique needs of institutions and cultures of groups, and explores the drivers, benefits, and value that time off can provide hospitalists. In this article, we share some of the highlights of the discussion.
Each of the panelists on the webinar shared that they have seen a cultural shift in the value hospitalists place on time off.
Dr. Gundareddy shared that, though his group has had PTO during his entire tenure at Johns Hopkins, in the last five years, they have seen a shift toward increasing utilization and most hospitalists using their full bank of PTO. He surmised that this is due to hospitalists needing additional flexibility to care for children and/or aging parents, combating burnout, and promoting wellness. He also noted that since COVID-19, there has been more self-awareness about the need to use sick time rather than show up for a shift unwell.
Dr. Shihadeh agreed and said that when her group switched from a Monday through Friday schedule to a seven-on, seven-off schedule, the importance of PTO increased. Additionally, she saw an increase in PTO utilization from about 40% pre-COVID-19 to now, with hospitalists using their entire PTO pool. Additionally, both Drs. Gundareddy and Shihadeh mentioned the role that PTO plays in allowing their foreign-born team members to visit or care for family.
Dr. Wills’ group does not offer PTO outside of federal and state regulations requiring paid time off for jury duty or family and medical leave (under the Family and Medical Leave Act). She reported that, when recruiting new hospitalists, recent conversations have been more focused on the group’s efforts to promote wellness rather than to focus solely on compensation.
Academic Teaching Hospital with PTO
At Johns Hopkins Bayview Medical Center in Baltimore, hospitalist faculty receive a bank of paid time off at the beginning of the academic year. This bank includes sick days, leaves of absence, and paid time off.
The group used its scheduling model to determine which clinical shifts needed continuity and created a cap system for how many hospitalists can be on PTO per day and for the volume of total PTO in a clinical block.
Hospitalists in the group don’t have to explain why they are using their PTO. “We realized internally [hospitalists] valued autonomy—autonomy in how they use their time and how their schedule looks. But then we also needed a functional schedule. So, we had to walk that fine line between flexibility and continuity. For a good PTO system to work, we had to understand how we can allow PTO to be used,” Dr. Gundareddy said.
For unexpected absences, a backup system was created, with one person on call who can cover the shift. The person activated is paid back in time during subsequent blocks, while the person calling out can use their PTO to cover for call-outs.
Additionally, the group uses part-time hospitalists, moonlighters, and historical data to build an additional buffer of full-time equivalents for longer breaks, such as the Family and Medical Leave Act or extended family emergencies.
Large Community Hospital with PTO
Hospitalists at Overlook Medical Center in Summit, N.J., accrue PTO over time, beginning after a 90-day waiting period upon hire, for a maximum of 17 to 18 days per year.
Physicians work 195 shifts in 15-day blocks for day shifts or 184 shifts as a nocturnist. Holiday schedules are released a year in advance, and any long stretches of PTO are requested six months in advance. There are some “gray out” days. For example, group members cannot take all their PTO between Thanksgiving and Christmas. The group has invested in a large per diem pool to cover unexpected absences and has no formal backup system. They generally have no issues covering shifts Monday through Friday and sometimes offer non-financial incentives, such as lower patient volumes, to those who cover shifts.
Large Academic Hospital with PTO Plan in Development
At Emory University and Grady Memorial Hospital in Atlanta, they are currently in conversation about what paid time off looks like for the group. The group has two daytime models: Monday through Friday and seven-on, seven-off. Continuity teams work 10-hour shifts, and they have dedicated nocturnists as well. To build flexibility, hospitalists can request days off four months in advance, and the scheduler is innovative in allotting time-off requests. Sometimes this results in hospitalists working more undesirable shifts, but they can take off the time requested.
For unexpected absences, the group has a jeopardy system for absences related to illness. For other absences, directors and leaders find coverage in the per diem pool or with locums.
All three panelists reported that there seems to be less of a coverage burden when team members do take PTO or call out. As taking time off has become more normalized, there is less sense of resentment among hospitalists when their teammates use their time off. The panelists all referenced their strong group morale as helping to cut through negative perceptions.
The webinar concluded with the panelists sharing how else they offer flexibility to their group. Hospitalists in their groups can leave when their work is done.
Additionally, all of them reported that when hospitalists on their team had a family emergency, they worked with them to find solutions so that they were able to be with their families. As Dr. Shihadeh said, “sometimes you have to do that for the good doctors that you have, [those] that you really want to retain.”

Ms. Caponiti

Dr. Gundareddy

Dr. Shihadeh

Dr. Wills
Ms. Caponiti is SHM’s practice management manager. Dr. Gundareddy is the associate division director for the division of hospital medicine at the Johns Hopkins Bayview Medical Center in Baltimore. Dr. Shihadeh is the section chief of the division of hospital medicine at the Overlook Medical Center in Northern New Jersey. Dr. Wills is an assistant professor in hospital medicine at Emory University’s division of hospital medicine at Grady Memorial Hospital, both in Atlanta.