
Children’s hospitals across the U.S. are increasingly experiencing capacity shortages, particularly at times of seasonal surges in acute illness.1 In addition, increasing closures of smaller and rural pediatric units have further consolidated pediatric beds to regional children’s hospitals, increasing bed demand.2 Our Pediatric Hospital Medicine service at Atrium Health Levine Children’s Hospital (AHLCH) in Charlotte, N.C., experiences ongoing capacity constraints. AHLCH spent more than 300 days (91%) at or near capacity during 2024, limiting access to care. Thus, the system searched for creative ways to expand capacity rapidly and control costs.
Solution Overview
At the height of the COVID-19 pandemic, hospital beds were in high demand. Many adult medicine services successfully adopted the hospital at home model, expanding acute care capacity by providing equivalent care in the comfort of the patient’s home. The model includes virtual monitoring by nurses and physicians, daily in-home paramedic or nurse visits, and the provision of services such as oxygen therapy, intravenous medication administration, and lab testing.3 Acute Hospital at Home (AH@H) has increased bed capacity, mitigated unintended consequences of hospital care such as traumatic experiences and increased family burden, and, in many cases, has decreased hospitalization costs.4-7
Our health system, Advocate-Atrium Health, has a large adult AH@H program operating successfully since the pandemic. This provided a framework to build upon. Through partnership with the adult AH@H leadership, we leveraged support for adaptation to a pediatric model with senior Atrium leadership. While pediatric AH@H is used in Europe and Australia for a variety of acute care issues, U.S. health systems have not integrated this model of care into pediatric medicine.8,9 Thus, with the international evidence of success in pediatrics and the success of our local adult AH@H program, our team saw pediatric AH@H as a viable solution for our pediatric bed capacity shortage.
In May 2024, we began the process of development and implementation of a full-service pediatric AH@H program that would allow us to demonstrate that this model can be adapted and successfully used in U.S. pediatric acute-care settings. Our goal was to demonstrate successful expansion of bed capacity while providing safe hospital care that is acceptable to patients, families, and practitioners.
Implementation Process
Beginning in May 2024, Atrium Health leadership brought together leaders from pediatric hospital medicine, nursing, paramedicine, pharmacy, ancillary services, and adult AH@H to begin pediatric AH@H implementation planning, background data collection, and evaluation design for the program. As the clinical program was designed, our evaluation team considered what data were needed to demonstrate that the program is safe and acceptable to both practitioners and families, as well as to evaluate the program rapidly throughout the implementation period and beyond. Together, these teams identified the initial patient populations served by this care model and how the program needed to be adapted for a pediatric population.
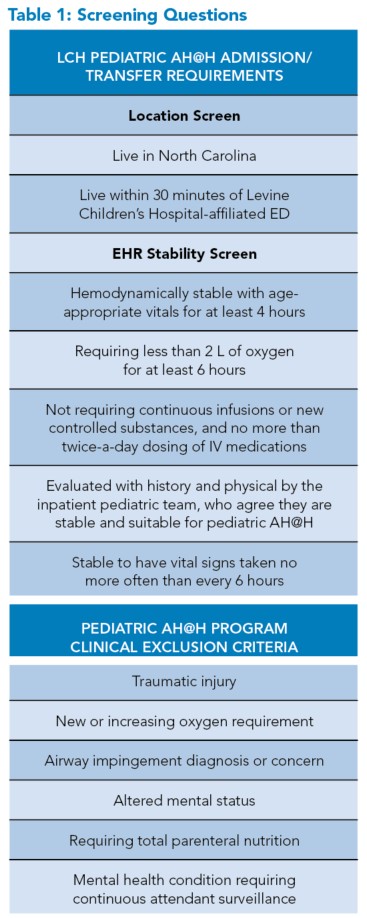
As program concepts developed, we recognized that the pediatric AH@H program would establish entry criteria that focused on patient stability instead of diagnosis, a distinction from the adult program. To meet the state-mandated regulatory requirements for our AH@H program, only patients in North Carolina and those within 30 minutes of our emergency department could be considered eligible.
We leveraged our adult paramedic service, known as Mobile Integrated Health, to identify a self-selected paramedic team that received additional training in pediatric care, including assessments, IV placements, and lab draws. We partnered with the adult AH@H and Levine Children’s Hospital (LCH) pediatric pharmacy teams to develop processes for medication verification, delivery, and subsequent in-home safety measures. Additionally, the Child Life department was brought on board early to design unique virtual care assistance and provide therapeutic and medical play items to the mobile units and families. Systems and flows for transferring to home, escalating care in home, and transferring back to the brick-and-mortar (BaM) hospital were all adapted from the adult program to fit the flow of our pediatric hospital service.
 |
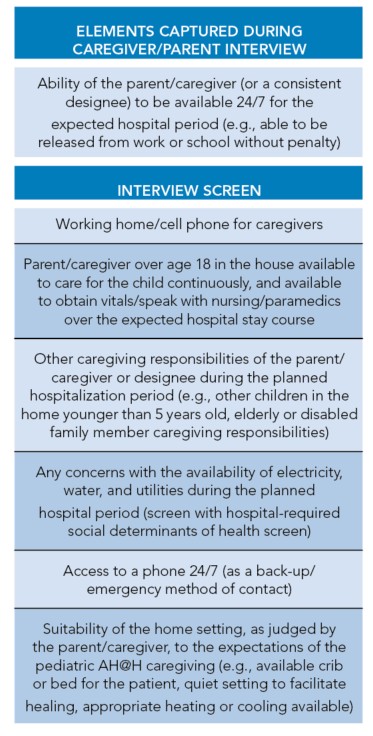 |
The program launched on February 3, 2025. For this novel program, patients are screened for medical stability (see Table 1). Those deemed stable, with permission from the BaM attending, are approached by a nurse navigator for a standardized interview to ensure the home environment and caregiver capacity are appropriate. Once the patient is screened in these two steps, they are offered care in pediatric AH@H.
Once enrolled, the patient transfers to the LCH-AH@H unit in the electronic health record (EHR), and transfer orders are placed by the pediatric AH@H clinician (see Figure 1). The paramedic team meets the family in the home after they travel there by private vehicle and sets up remote two-way monitoring systems, and the patient has the first virtual visit. Patients are seen in person by the paramedic, virtually by the hospitalist, and by the pediatric nurse twice daily until discharge from the program. Families have virtual access to their nurse and physician 24 hours a day.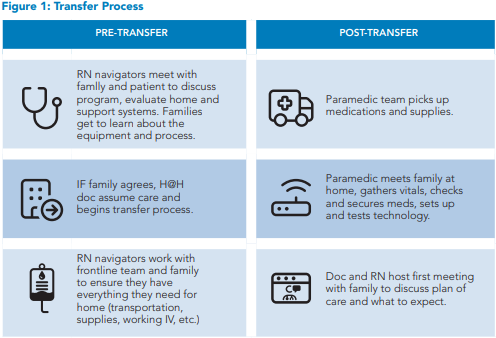
Equipment can be a challenge in the pediatric AH@H setting, as the market for this type of equipment has been adult-focused until recently, and many companies are just moving into the pediatric-population market. The equipment for remote patient monitoring and communication used by our adult program is approved by the U.S. Food and Drug Administration for patients 14 and older. Thus, we had to develop a research protocol with the vendor to use communication equipment for patients younger than 14 years, and we have had delays in sourcing remote monitoring equipment approved for use in children of all ages. This has led to delays in enrolling younger children who require continuous vital sign monitoring.
Obtaining the buy-in of our hospitalists required continuous ongoing engagement, with frequent updates on program development in 2024 and on enrollments and metrics once launched in 2025. The AH@H team actively screens patients and reaches out to the BaM teams with potential candidates. This allowed gradual growth in the understanding of potential candidates for the program. In addition, care was taken not to increase the BaM teams’ workload in that all transfer orders and arrangements are made by the AH@H team.
An additional obstacle we considered when building out the program was the ability to communicate with non-English-speaking families. The virtual platform we use provides auto-translation from English to Spanish and vice versa in the chat function. This is critical for nurse-family communication when not on a video call. We have access to virtual interpreters, but have not yet enrolled patients who do not speak English or Spanish due to the limitations.
Outcomes
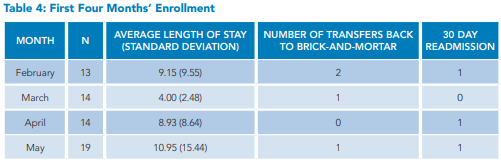
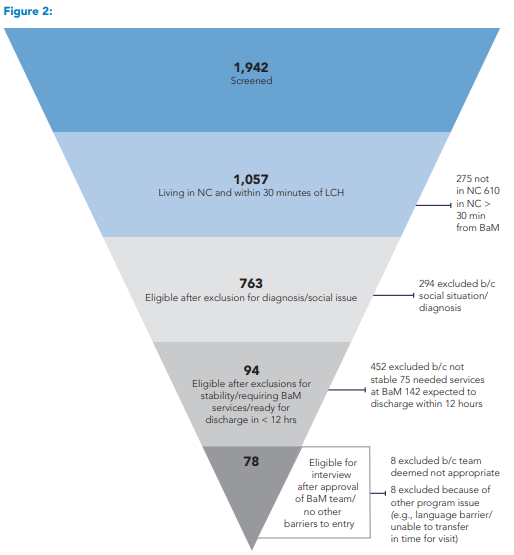 Since the start of the program, we have screened 1,942 patients admitted to the hospitalist service. Figure 2 illustrates the flow of patients through the screening to the point of qualifying for an eligibility interview. We interviewed 78 families. All were deemed eligible after the interview. Of these, 57 consented to enter the program. Table 2 lists the reasons families declined entry into the program, Table 3 summarizes the age ranges of patients in the program, and Table 4 shows enrollments by month.
Since the start of the program, we have screened 1,942 patients admitted to the hospitalist service. Figure 2 illustrates the flow of patients through the screening to the point of qualifying for an eligibility interview. We interviewed 78 families. All were deemed eligible after the interview. Of these, 57 consented to enter the program. Table 2 lists the reasons families declined entry into the program, Table 3 summarizes the age ranges of patients in the program, and Table 4 shows enrollments by month.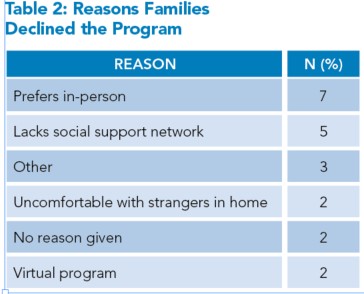
The three most common reasons for hospitalization in pediatric AH@H were dehydration, feeding difficulty, and treatment of infection. Overall, patients have been satisfied with the service to date, exceeding our patient satisfaction scores for our BaM units. Given the limited number of clinicians involved in the program, surveys have not yet been distributed to staff. Over the five months, we have seen increases in referrals to the unit by members of our BaM hospitalist team. Given that the program has not reached a steady state, the calculation of bed days saved per patient in pediatric AH@H has not yet been reported. If these BaM beds are backfilled with traditional pediatric hospital patients, a projected return on investment will be calculated.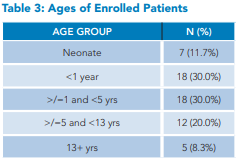
Lessons Learned
This novel approach to pediatric care, born out of a bed capacity shortage, embraced innovation and focused on the unique needs of pediatric patients while leveraging in-house resources from a robust adult AH@H program. We demonstrated that through careful process planning, thoughtful design of inclusion and exclusion criteria, and partnership, pediatric AH@H is implementable. As technology is optimized for remote patient monitoring, designing and obtaining Food and Drug Administration approval for such technology must include children of all ages.
While we are the largest quaternary children’s hospital in our state, we are not strictly a standalone children’s hospital. Thus, we were able to take advantage of the larger system’s hospital-at-home waiver for reimbursement of services, functionally helping us launch within an expedited timeline and with a template for reimbursement. For sustainability, there is a need to demonstrate clear value from the perspectives of patients and families, the health system, and staff. This will require well-designed evaluations of these program aspects. Creating a compelling argument for both waivered and non-waivered viability of this care model is essential for pediatric hospitals across the U.S. that face capacity constraints.
Future Directions
Pediatric AH@H represents a real step forward in patient-centered pediatric acute care. We are actively planning the expansion of the service across all the pediatric centers served by our hospitalist team, and then across other children’s centers in our healthcare system.
As we consider the declining pediatric subspecialty practitioner numbers, we are planning to work in collaboration with subspecialists to develop pathways for specific patient populations that may be well-served by this model. Pediatric AH@H has immense potential as a viable care model for special populations, including late preterm infants and postoperative and complex-care patients. Evaluating the efficiency of program entry, hours for entry, and the timing and frequency of patient visits is necessary to allow more patients access to this model. For example, we can only deliver twice-daily IV medication in our current model. Having the ability to do IV medication three times a day will allow many more children to qualify. We are also planning to compare patient outcomes for those cared for in this new model with BaM standards, as a crucial component in ensuring that high-quality inpatient care can be delivered reliably in this new way.
|
Dr. Obita is a pediatric hospitalist at Atrium Health Levine Children’s Hospital and associate professor of pediatrics at Wake Forest University School of Medicine, both in Charlotte, N.C. |
Dr. Reed is a pediatric hospital medicine faculty member, site director for pediatric hospital medicine, and medical director of the first U.S., comprehensive, acute-care, pediatric, hospital-at-home program at Atrium Health Levine Children’s Hospital, and assistant professor of pediatrics at Wake Forest University School of Medicine, both in Charlotte, N.C. |
Dr. Horstmann is a pediatric hospitalist at Atrium Health Levine Children’s Hospital, an associate professor of pediatrics at Wake Forest School of Medicine, and the division director of pediatric hospital medicine at Atrium Health, all in Charlotte, N.C. |
Dr. Dodds is a pediatric hospitalist at Atrium Health Levine Children’s Hospital and assistant professor of pediatrics at Wake Forest University School of Medicine, both in Charlotte, N.C. |
|
Dr. Marseille is a pediatric hospitalist at Atrium Health Levine Children’s Hospital, and assistant professor of pediatrics at Wake Forest University School of Medicine, both in Charlotte, N.C. |
Dr. Long is an associate professor of biostatistics and data science at Wake Forest School of Medicine in Winston-Salem, N.C. |
Dr. Liu is a data scientist with the Research and Excellence in Advancing Children’s Health program at Atrium Health Levine Children’s Hospital in Charlotte, N.C., and an adjunct assistant professor of biostatistics and data science at Wake Forest University School of Medicine in Winston-Salem, N.C. |
Dr. Turley is the vice chair for research at Atrium Health Levine Children’s Hospital and professor of pediatrics at Wake Forest University School of Medicine, both in Charlotte, N.C. |








Key Points
- Pediatric AH@H can be implemented in a U.S. children’s hospital.
- Careful planning to determine suitable populations is important, and focusing on patient characteristics over diagnoses allows for more potential access to the service.
- For growth in this model, key aspects of sustainability and appropriate equipment will be needed
References
1. Leyenaar JK, et al. Pediatric hospitalizations at rural and urban teaching and nonteaching hospitals in the US, 2009- 2019. JAMA Netw Open. 2023;6(9):e2331807. doi: 10.1001/ jamanetworkopen.2023.31807.
2. Cushing AM, et al. Availability of pediatric inpatient services in the United States. Pediatrics. 2021;148(1):e2020041723. doi: 10.1542/peds.2020-041723.
3. Leff B. Defining and disseminating the hospital-at-home model. CMAJ. 2009;180(2):156-7. doi: 10.1503/cmaj.081891.
4. Cryer L, et al. Costs for ‘hospital at home’ patients were 19 percent lower, with equal or better outcomes compared to similar inpatients. Health Aff (Millwood). 2012;31(6):1237- 43. doi: 10.1377/hlthaff.2011.1132.
5. Federman AD, et al. Association of a bundled hospital-at-home and 30-day postacute transitional care program with clinical outcomes and patient experiences. JAMA Intern Med. 2018;178(8):1033-1040. doi: 10.1001/jamainternmed.2018.2562.
6. Leff B, et al. Hospital at home: feasibility and outcomes of a program to provide hospital-level care at home for acutely ill older patients. Ann Intern Med. 2005;143(11):798- 808. doi: 10.7326/0003-4819-143-11-200512060-00008.
7. Levine DM, et al. Acute hospital care at home in the United States: the early national experience. Ann Intern Med. 2024;177(1):109-110. doi: 10.7326/M23-2264.
8. Detollenaere J, et al. Systematic literature review on the effectiveness and safety of paediatric hospital-at-home care as a substitute for hospital care. Eur J Pediatr. 2023;182(6):2735-2757. doi: 10.1007/s00431-023-04916-2.
9. Sump C, et al. Hospital at home for children: an emerging model of acute care. Hosp Pediatr. 2024;14(2):e110-e112. doi: 10.1542/hpeds.2023-007441