
Staffing shortages in hospital medicine affect hospitals nationwide, presenting a critical challenge. The Association of American Medical Colleges projects a shortage of up to 86,000 physicians by 2036.1 Hospitalist positions remain hard to fill, with vacancy rates ranging from 7% to 20% depending on the region.2 Rural communities are more severely affected, including within the Veterans Health Administration (VHA), where 96% of rural VHA hospitals reported inpatient staffing vacancies in 2019.3
Rural VHA hospitals serve a critical need for millions of veterans living in rural areas, allowing them to receive care closer to their homes and support systems, which results in better outcomes.4,5 Yet, maintaining inpatient staffing around the clock is challenging and costly. Moreover, VHA hospitals often have large campuses that include regular inpatient units, nursing homes, inpatient rehabilitation, psychiatry units, and long-term care, which amount to a large physical footprint, creating additional challenges for 24/7 coverage.
Solution Overview
The VA National Tele-Hospital Medicine (Tele-HM) program was created in 2019 as an innovative staffing model to support rural VHA hospitals. The pilot program supporting one site during the daytime showed high care-team acceptance and decreased length of stay.6
The Tele-HM Cross-Coverage Model
Given the critical need of many facilities for additional staffing support during weekends, holidays, evenings, and nighttime hours (often referred to as “WHEN” hours), the Tele-HM program implemented a gradual expansion to provide cross-coverage support to multiple rural VHA hospitals. With support from the Office of Rural Health’s Enterprise-Wide Initiative, or EWI, program, Tele-HM cross-coverage services launched in the summer of 2023, serving just two hospitals initially with weekend and holiday service, and expanded to night coverage in September 2024. Similar night coverage models have been described in the community setting and have gained popularity among critical-access hospitals.7
The program’s primary objectives included:
- Providing 24/7 access to high-quality, timely, hospital medicine expertise for rural veterans admitted to rural VA facilities
- Supporting the workforce at rural VHA hospitals with schedule flexibility
- Expanding system capacity and reducing the need for community care utilization
- Reducing staffing inefficiencies and optimizing workforce utilization
- Decreasing unnecessary escalations of care for after-hours evaluations
Given that a single telehospitalist can provide support to several facilities simultaneously, Tele-HM allows local practitioners to focus on the care of the most critically ill patients, while the telehospitalist can provide support for less acute patients, cross-coverage needs, and after-hours admissions. The model then promotes more efficient staffing structures, allows for built-in surge capacity, and promotes staff retention of on-site hospitals that can decrease their night coverage.
Implementation Process
The Tele-HM program is comprised of a national network of experienced, board-certified, Veterans Administration (VA) hospitalists, a nurse coordinator, and an administrative team. The VA Tele-HM hub is hosted by the Iowa City VA Healthcare System, and experienced hospitalists from across the country deliver care, leveraging the 2018 VA’s “Anywhere to Anywhere” initiative that allows VA doctors and other healthcare clinicians “to administer care to veterans using telehealth, or virtual technology, regardless of where in the United States the provider or veteran is located, including when care will occur across state lines or outside a VA facility.”8
Tele-HM uses the simplest technology possible to achieve the goal of delivering high-quality care. As such, only a modest upfront investment is needed to deploy the program, including video-capable, portable devices at the patient site, a tele-stethoscope, and optional peripherals (high-resolution camera, digital otoscope, etc.). Tele-HM practitioners access electronic health records, perform assessments via synchronous video telehealth secure portal, and collaborate with onsite nurses, tele-presenters, or practitioners (trainees, nurse practitioners, physician assistants, or non-medical specialists) to obtain all the relevant information and provide comprehensive care.
The Tele-HM cross-coverage model involves a three-phase implementation:
1. Pre-implementation (two to four months before go-live): During this phase, local teams in collaboration with the Tele-HM leadership meet regularly to identify the need for and the scope of services, complete administrative and credentialing processes, develop clinical protocols, procure equipment, and educate both “spoke” site and Tele-HM staff. Pre-implementation interviews with key local staff, and (if possible) site visits were conducted to learn about perceptions and attitudes toward the Tele-HM program, discover any anticipated challenges, build trust among teams, and facilitate the development of clinical care processes.
2. Implementation phase (go-live): This includes simulation and launching the selected service model. Currently, the VA Tele-HM program offers three models of care:
- Cross-coverage support: providing after-hours coverage and attending to the needs of patients admitted to VA acute, subacute, or residential settings
- Primary telehospitalist staffing: independently completing admissions, triages, and consults with the assistance of an on-site nursing staff or a tele-presenter
- Team-based care model: Tele-HM providing oversight or consultation of trainees or advanced practice practitioners
Facilities can select the service model based on their needs and local resources. During the shifts, Tele-HM clinicians have direct communication with the spoke sites using an online secure platform, conduct video visits for patient evaluations, place orders, and document in the chart. Written and verbal hand-off between Tele-HM providers and on-site practitioners allows for seamless transitions and optimal continuity of care.
3. Post-implementation phase: Tele-HM leadership teams and spoke site leaders join ongoing programmatic calls to facilitate continuous process improvements, identify any issues, and modify protocols based on changing needs. The Tele-HM team or the spoke sites will suggest opportunities for care process improvements if identified. Post-implementation surveys are also distributed to the spoke site staff, and veterans served at regular intervals to assess satisfaction with the program.
Outcomes and Impact
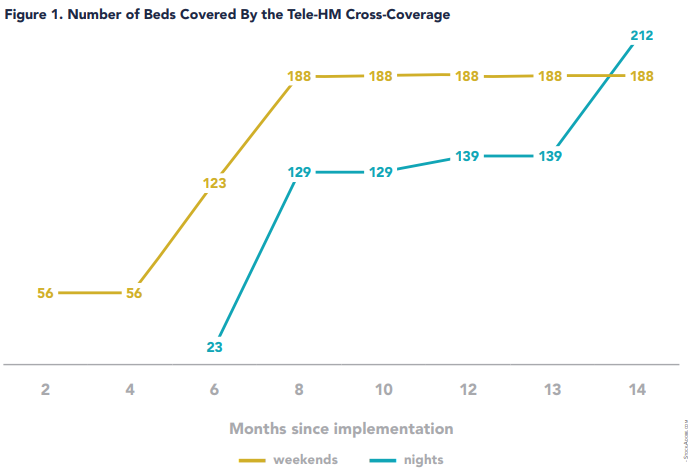
Since 2019, the VA Tele-HM program has grown to meet the needs of rural veterans, implementing services at 11 rural VHA hospitals across eight states. The services have completed more than 7,500 patient encounters for more than 2,500 veterans. Six VHA hospitals have adopted the Tele-HM cross-coverage model in the past two years, with one more in the queue. Almost 6,000 hours of coverage for nights, weekends, and holidays have been provided to the Tele-HM cross-coverage spoke sites, and the practitioners have completed more than 1,300 clinical contacts.
The number of beds covered by the program has rapidly increased both for weekend and nighttime hours, as shown in Figure 1.
Veteran experience with the program has been overwhelmingly positive. Of 120 post-discharge patient phone surveys completed (180 attempted, 67% response rate) by veterans who interacted with the program, 96% were satisfied or very satisfied with the care they received during the hospitalization, 95% agree or strongly agree that telehospitalist practitioners managed their care well, more than 90% reported excellent communication skills for the practitioners, including explaining things in ways the patient could understand and listening attentively to their concerns, and 95% did not report any issues with the technology or connectivity.
On-site care teams have reported the program’s positive impacts: staffing and scheduling flexibility, built-in surge capacity, leave coverage, increased retention and job satisfaction for on-site staff, and significant cost savings.
Tele-HM cross-coverage has resulted in cost reductions of an average of $600,000 annually in savings per site and allowed for a reduction of an average of two full-time equivalent (FTE) onsite clinicians, without affecting access or timeliness of veteran care. In addition, partner sites have reported significant reductions in unnecessary escalations of care to the emergency department or inpatient units from the nursing homes or residential programs. These quantifiable successes illustrate the program’s effectiveness in improving access, quality of care, and operational efficiency while reducing costs.
With the increasing need to optimize access to care, increased shortages of hospitalists nationwide, and ongoing efforts to reduce costs, telehospitalist programs, and in particular the telehospitalist cross-coverage model, offer a sustainable solution for federal agencies and multi-site healthcare systems. By covering multiple sites simultaneously, it optimizes workforce utilization, bed capacity, reduces external transfers, and facilitates the adoption of best practices across multiple sites. Given that federal physicians can deliver care across state lines, and the fact that the VHA has been a pioneer in the development and adoption of telehealth programs, the VHA is a prime environment to expand this model. With a national reach, the program can continue to help the VHA to share its hospitalist workforce across the enterprise to support the more than 130 VA hospitals, serving more than nine million veterans. Lessons from the program can be extrapolated to other multi-site healthcare systems with growing footprints and increased need for efficiency.
Lessons Learned
Flexibility is a key aspect of program development and implementation. Despite the VA being a national healthcare system, each facility has a series of unique and specific needs. A key driver of success for the program has been striking a balance between meeting sites’ unique needs and standardizing processes across sites to allow scalability.
Continuous stakeholder engagement and local clinical champions are important. Clinical champions help inform clinical processes, ensure they are appropriate for the local context, and anticipate potential barriers, while stakeholders align goals and vision for the program and effectively communicate with their teams.
Pre-implementation site visits facilitate deployment and increase trust. Direct observation of local resources, processes, and operations by the Tele-HM team facilitated the development of more comprehensive training materials for the Tele-HM staff and helped build trust with the partner spoke site.
Ongoing feedback ensures sustainability. Adjustments and modifications based on outcomes, feedback, and changes in need are critical to sustainment.
Disseminating best practices expands quality improvement. Many Tele-HM providers are academic hospitalists, which has helped to disseminate evidence-based practices more expeditiously to rural facilities. For example, Tele-HM team members participated in a nationwide task force to improve alcohol withdrawal syndrome treatment across the VHA.
A strong administrative team and internal communication mechanisms are critical. Program administrative support helps to ensure seamless deployment and implementation. Strong internal communication channels and robust training materials allow the program to keep practitioners continuously up to date, which promotes ongoing success. The VHA Tele-HM cross-coverage model adds to the body of evidence that telehealth use for after-hours hospitalist care is feasible, safe, and cost-effective.7,9
Future Directions
Future steps include expanding the Tele-HM service to more VHA hospitals across the country; providing surge capacity for rural and urban facilities, emergency coverage, and disaster response; and even expanding to sites outside the VHA to facilitate consultations and care coordination for veterans admitted to community hospitals.
Tele-HM is also exploring further technological enhancements to improve service delivery, including a pilot technology solution for triaging requests from different sites, which will allow the program to further streamline communication and reduce response times. The program aims to extend its reach while continuing to refine processes for even greater efficiency and effectiveness.
Acknowledgments: Thanks to: Our spoke and partner sites for their ongoing collaboration and trust in our model; our administrative team, Judith Vinzant and Melissa Lestina, for their role in successful program implementation, training, and ongoing communications with sites and providers; the Tele-HM evaluation team, George Bailey, Jacqueline Benson, Octavia Goodman, Tracy Moffett, Robert Burke, and Charlie Wray, for their role in data collection; and lastly, we thank Dr. Sailaja Bandi for her input and review of this paper. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government. Funding: Department of Veterans Affairs, Veterans Health Administration, Office of Rural Health, NOMAD #PROG-0000111

Dr. Gutierrez

Dr. Cohen

Dr. Jindal
Dr. Gutierrez is a clinical associate professor of internal medicine, interim division director of hospital medicine at the University of Iowa Carver College of Medicine in Iowa City, Iowa, and the director of the VA National TeleHospital Medicine program. Dr. Cohen works for the VA Clinical Resource Hubs in more remote and complex areas of the U.S., where there are gaps in coverage (primary care, specialty care, urgent, emergency, and hospital medicine care). Dr. Cohen delivers primary, urgent, emergency, and hospital medicine care across the VA system, extending her reach to multiple sites through coordinated telehealth systems and team-based models of care, bringing years of academic clinical experience to these sites while expanding access to resource limited areas of the U.S. Dr. Jindal is a hospitalist and section chief for hospital medicine at the Veterans Affairs New York Harbor Healthcare System, Manhattan campus, and an assistant professor in the department of medicine at NYU Grossman School of Medicine, both in New York, and deputy director of the VA National TeleHospital Medicine program.
Key Points
- The Tele-HM cross-coverage program is revolutionizing rural veteran care by providing high-quality on-demand hospitalist physician expertise 24/7.
- The program ensures continuous access to care at rural VA medical centers despite severe staffing shortages.
- By covering multiple facilities simultaneously, the Tele-HM program optimizes hospitalist workforce utilization across the VHA, reduces external transfers, and facilitates the dissemination of best practices across the VHA.
- This model can be used by other healthcare systems providing services to smaller and rural hospitals with low patient volume to increase staffing efficiency while maintaining access to care.
- Future directions include expanding the model and leveraging technology solutions to optimize triage and communication functions.
References
1. GlobalData Plc. The complexities of physician supply and demand: projections from 2021 to 2036. AAMC website. https://www.aamc.org/media/75236/download. Published March 2024. Accessed October 29, 2025.
2. Society of Hospital Medicine (SHM) Practice Analysis Committee. 2023 state of hospital medicine report. Available at: https://www.hospitalmedicine.org/practice-management/2023-sohm/. [Paywall]. Published 2023. Accessed October 29, 2025.
3. Moeckli J, et al. Perceived need and potential applications of a telehospitalist service in rural areas. Telemed J E Health. 2021;27(1):90-95. doi: 10.1089/tmj.2020.0018.
4. Yoon J, et al. Outcomes of veterans treated in Veterans Affairs hospitals vs non-Veterans Affairs hospitals. JAMA Netw Open. 2023;6(12):e2345898. doi: 10.1001/jamanetworkopen.2023.45898.
5. Apaydin EA, et al. Veterans Health Administration (VA) vs. non-VA healthcare quality: a systematic review. J Gen Intern Med. 2023;38(9):2179-2188. doi: 10.1007/s11606-023-08207-2.
6. Gutierrez J, et al. Implementing a telehospitalist program between Veterans Health Administration hospitals: outcomes, acceptance, and barriers to implementation. J Hosp Med. 2021;16(3):156-163. doi: 10.12788/jhm.3570.
7. Eagle Telemedicine. Night coverage solutions: why they work for hospitals and physicians. Eagle telemedicine website. http://www.eagletelemedicine.com/wp-content/uploads/2016/11/EHP_WP_ Telenocturnist_FINAL.pdf. Published 2016. Accessed October 29, 2025.
8. US Department of Veterans Affairs. News release: VA expands telehealth by allowing health care providers to treat patients across state lines. VA website. https://www.va.gov/opa/pressrel/includes/viewPDF.cfm?id=4054. Published May 11, 2018. Accessed October 29, 2025.
9. Sanders RB, et al. New hospital telemedicine services: potential market for a nighttime telehospitalist service. Telemed J E Health. 2014;20(10):902-8. doi: 10.1089/ tmj.2013.0344
Is there a ratio of telehospitalist to number of beds covered that is being utilized to keep staffing appropriate? Are you able to share what ratios have been used to adjust staffing?